909
Views & Citations10
Likes & Shares
Background: Micro-TESE
(Microdissection testicular sperm extraction) is a best technique of sperm retrieval for non-obstructive
azoospermic patients. This study is carried out to evaluate the possibility of
successful retrieval of sperm and the relation of its sperm retrieval rate with
patients' characteristics.
Materials and methods:
We
surveyed50 patients with non-obstructive azoospermia who underwent micro-TESE
from June 2016 to July 2017 at Centre for Assisted Reproduction, Vietnam
Military Medical University. Medical documents were reviewed for the outcome of
the average patients' age, duration of infertility, testicular volume, follicle
stimulating hormone (FSH), luteinizing hormone (LH), testosterone levels, AZF
microdeletions analysis and the overall sperm retrieval rate.
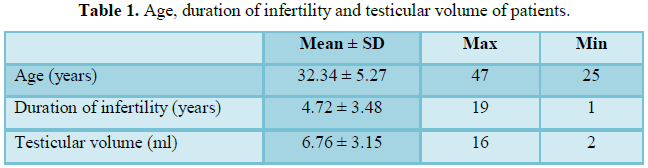
Results: The average
patients' age was 32.34 ± 5.27 years, duration of infertility 4.72 ± 3.48 years;
testicular volume 6.76 ± 3.15 ml. Six (12%) patients had AZF microdeletions.
Patients' age, testicular size, serum LH, testosterone and AZF microdeletions
showed no significant effect on sperm retrieval rate. FSH levels differ
significantly in patients with whom sperm is retrieved versus patients where
sperm is not retrieved with micro TESE. The overall sperm retrieval rate was
32%.
Conclusion: Microdissection
testicular sperm extraction (micro-TESE) has a high sperm retrieval rate. FSH
levels may be able to foretell the possibility of getting spermatozoa in
patients with non-obstructive azoospermia.
Keywords: Microdissection
testicular sperm extraction, Non-obstructive azoospermia, Sperm retrieval
INTRODUCTION
Azoospermia is explained
as the lack of spermatozoa in the ejaculate after the assessment of centrifuged
semen on at least two occasions. It is noticed in 1% of the general population
and in 10%-15% of infertile men [1].
Surgical sperm
retrieval and intracytoplasmic sperm injection (ICSI) have revolutionized the
management of non-obstructive azoospermia (NOA) [2]. Fine-needle aspiration
(FNA), percutaneous testis biopsy and open testicular biopsy or testicular
sperm extraction (TESE) can be used to retrieve testicular spermatozoa [3].
Failure to extract spermatozoa may happen
in up to 57% of TESE attempts [4]. Focal testicular spermatogenesis
accounts for the failure rate of these procedures [5]. Moreover, multiple testicular biopsies can ensue in the loss of
testicular tissue and can interrupt the testicular blood supply underneath the
tunica albuginea with uncertainty of testicular devascularization and atrophy
of the testis [6]. Microdissection TESE (micro-TESE) was introduced to try to
sample focal healthy looking tubules, thus to maximize the yield of
spermatozoa, lessen the amount
of testicular tissue removed, make sperm retrieval rate (SRR) better and keep away from subtunical vessels [7].
We performed the study to evaluate the possibility of successful retrieval of sperm and the relation of
its sperm retrieval rate with patients' characteristics.
MATERIALS AND METHODS
Study population
This study was approved by the institutional review board of
We surveyed 50 patients with non-obstructive azoospermia with healthy
female partners who had undergone micro-TESE from June 2016 to July 2017 at
Centre for Assisted Reproduction, Vietnam Military Medical University.
All patients were diagnosed on the basis of a complete history, physical
examination, and endocrine profile. Medical documents were evaluated for
follicle stimulating hormone (FSH), luteinizing hormone (LH), total
testosterone levels, AZF analysis. Testicular volume was taken the
measurements with a Praderorchidometer.
Seminal study
Semen samples were made by masturbation after 3-5 days of sexual
abstinence and gathered into
sterile containers. The presence of azoospermia was recorded in at least two semen specimens more than 2 weeks apart,
all processed with centrifugation at 3000 g and extensive examination of the re-suspended
pellet. A repeat analysis was also carried out on the morning of the planned
sperm retrieval.
Hormonal measurements
Serum FSH, LH and total testosterone were taken the measurements and documented preoperatively, at 3 months
(early) and more than 1 year (late) follow up visits.
Screening method for AZF
microdeletions
Polymerase chain reaction (PCR) amplification using specific
sequence-tagged sites (STS) was carried out to screen for AZF region
microdeletions of the Y chromosome.
Microdissection testicular sperm extraction
Procedures were carried out under regional anesthesia, with the patient
positioned on an operating table in a supine position. The operating microscope
(Karl Zeiss, Germany) was used throughout the procedures. After skin
disinfecting and draping, the scrotal skin was stretched over the anterior surface
of the testis and a 2.5 cm midline raphe longitudinal incision was placed. The
incision was performed through the dartos muscle and tunica vaginalis. The
tunica was opened and its bleeders cauterized. The testis was taken extra vaginally
and the tunica albuginea was examined. A single large longitudinal intra-polar
incision was made on an avascular area in the tunica albuginea under 6-8x
magnification and the testicular parenchyma was widely revealed. Dissection of the testicular parenchyma was then undertaken
at 16-25x magnifications searching for enlarged tubules, which are more likely
to have capacity for germ cells. The superficial and deep testicular regions
were inspected, as needed, and microsurgical-guided
testicular biopsies were carried out by carefully removing enlarged and opaque
tubules using microsurgical forceps. If enlarged tubules were not seen, then
two to three random micro-biopsies were carried out at the upper, medium and
lower testicular poles. The excised specimens were put into the center well of petri
dishes containing phosphate-buffered saline (PBS) in room temperature and
processed as described below. The tunica albuginea was closed using continuous
non-absorbable 5-0 polydioxanone sutures suture. Following hemostasis, the
tunica vaginalis was closed in a running fashion using similar suture, after
that the dartos muscle was closed with interrupted Vycril sutures. Eventually, the skin was closed with
continuous subcuticular 5-0 monocryl suture and a fluffy-type dressing and
scrotal supporter were put. The procedures were performed at the contralateral
testicle, as needed, when an insufficient number or no sperm have been found at
initial laboratory examination. Patients were discharged same day of surgery.
Success was explained as the
presence of a sperm that could be either preserved or used for ICSI.
Tissue processing and sperm retrieval
Testicular tissues obtained at the procedure were put into 2 ml of PBS
medium supplemented with 0.8 mg/ml collagenase Type IA (Sigma). The tissue samples
were digested in an incubator at 37°C for 2 h. To facilitate complete enzymatic
digestion, the samples were vibrated
every 10-15 min during this incubation period. The cell suspension
(supernatant) having capacity for the loose cells was then cleaned with PBS medium and
centrifuged for 10 min at 2000 g. The supernatant was removed and the pellet re-suspended
in 50-100 μl. A drop of 5 μl from each of the suspensions representing one
biopsy was taken for examination on a glass slide with coverslip under a
microscope.
STATISTICS
Descriptive statistics were illustrated as the mean (standard
deviation) and percent. The value of p<0.05 was considered statistically
significant for all tests carried out using the Predictive Analysis Software
version 19.0 (SPSS Inc., IBM, Chicago, Illinois, USA).
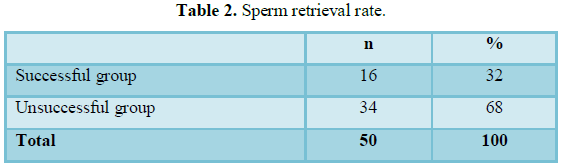
RESULTS
The sperm retrieval
was successful in 16 (32%) patients and unsuccessful (no sperm found) in 34
(68%) patients (Table 2).
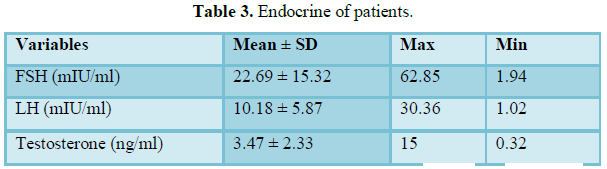
Their average serum
FSH, LH and testosterone were 22.69 ± 15.32 mIU/ml, 10.18 ± 5.87 mIU/ml and 3.47 ± 2.33 ng/ml (Table
3).
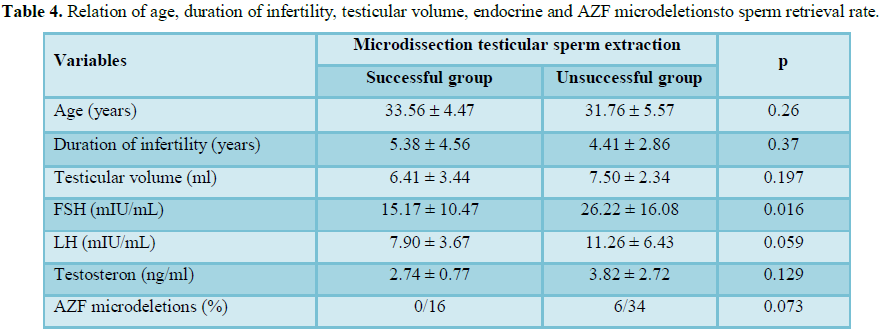
Patients' age, duration
of infertility, testicular size, serum LH, testosterone and AZF microdeletions showed
no significant effect on sperm retrieval
rate. But FSH levels may be able to foretell
the possibility of
getting spermatozoa in patients with non-obstructive azoospermia
(p=0.016) (Table 4).
DISCUSSION
The introduction of ICSI and the application of different testicular
sperm retrieval techniques have revolutionized treatment in patients with NOA
[2]. Different methods can be used to retrieve testicular spermatozoa, including
FNA, open testicular biopsy and percutaneous biopsy [3]. The introduction of
micro-TESE has made sperm retrieval rate better, maximized the yield of
spermatozoa per biopsy, resulted in removal of less testicular tissue and had
fewer acute and chronic complications than conventional procedures [8].
Sperm retrieval rate between 33.3% and 63% have been notified after
micro-TESE [9,10]. In our series, sperm retrieval rate was 32%. Serum FSH can
be used as predictive factors of success. Our outcome concur with previously
published studies that showed patients' age, duration of infertility,
testicular size, serum LH, testosterone and AZF microdeletions had no effect on
sperm retrieval rate (Table 4).
Our study had some
limitations. First, there were only a limited number of patients, limited
number of relevant studies, so we analysed some parameters as predictors for sperm retrieval rate, such as average patients' age, duration of
infertility, testicular volume, follicle stimulating hormone (FSH), luteinizing
hormone (LH), testosterone levels, AZF microdeletions. Second, the
measurement methods and reference levels of both FSH and testicular volume
varied among different studies, which might have an effect on the results of our analysis.
This is the first study evaluating the possibility of successful retrieval of sperm on Microdissection testicular sperm extraction in non-obstructive
azoospermic Vietnamese. In this study, the testicular tissue samples were
digested by collagenase Type IA (0.8 mg/ml). The enzymatic digestion process
take a long time but this process is easy to perform, and does not damage
cells.
CONCLUSION
Micro-TESE (Microdissection testicular sperm extraction) has a high
sperm retrieval rate (32%), minimal postoperative complications. Patients' age,
duration of infertility, testicular size, serum LH and testosterone showed no
significant effect on sperm retrieval rate. FSH levels may be able to foretell
the possibility of getting
spermatozoa in patients with non-obstructive azoospermia.
1.
Jarow
JP, Espeland MA, Lipshultz LI (1989) Evaluation of the azoospermic patient. J Urol 142:
62-65.
2. Devroey P, Liu
J, Nagy Z, Goossens A, Tournaye H, Camus M, et al. (1995) Pregnancies after testicular sperm extraction
and intracytoplasmic sperm injection in non-obstructive azoospermia. Hum Reprod
10: 1457-1460.
3. Friedler S, Raziel A, Strassburger D, Soffer
Y, Komarovsky D, et al. (1997) Testicular sperm retrieval by percutaneous fine
needle sperm aspiration compared with testicular sperm extraction by open
biopsy in men with non-obstructive azoospermia. Hum Reprod 12: 1488-1493.
4. Schlegel PN, Palermo GD, Goldstein M,
Menendez S, Zaninovic N, et al. (1997) Testicular sperm extraction with
intracytoplasmic sperm injection for non-obstructive azoospermia. Urology 49:
435-440.
5. Silber SJ (2000) Microsurgical TESE and the
distribution of spermatogenesis in non-obstructive azoospermia. Hum Reprod 15:
2278-2284.
6. Schlegel PN, Su LM (1997) Physiological
consequences of testicular sperm extraction. Hum Reprod 12: 1688-1692.
7. Schlegel PN (1999) Testicular sperm
extraction: Microdissection improves sperm yield with minimal tissue excision.
Hum Reprod 14: 131-135.
8. Amer M, Ateyah A, Hany R, Zohdy W (2000)
Prospective comparative study between microsurgical and conventional testicular
sperm extraction in non-obstructive azoospermia: Follow-up by serial ultrasound
examinations. Hum Reprod 15: 653-656.
9. Tsujimura A, Miyagawa Y, Takao T, Takada S,
Koga M, et al. (2006) Salvage microdissection testicular sperm extraction after
failed conventional testicular sperm extraction in patients with non-obstructive
azoospermia. J Urol 175: 1446-1449.
10. Everaert K, De Croo I, Kerckhaert W, Dekuyper
P, Dhont M, et al. (2006) Long term effects of micro-surgical testicular sperm
extraction on androgen status in patients with non-obstructive azoospermia. BMC
Urol 6: 9.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Allergy Research (ISSN:2642-326X)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Pathology and Toxicology Research


